You've been told your iron is "a bit low" and handed a supplement. So you take it. Weeks pass. Nothing really changes. That is probably because there is a whole lot more to your iron status than what your pathology tests are telling you!
Sound familiar? If it does, there's a good chance the real problem is sitting below the surface.
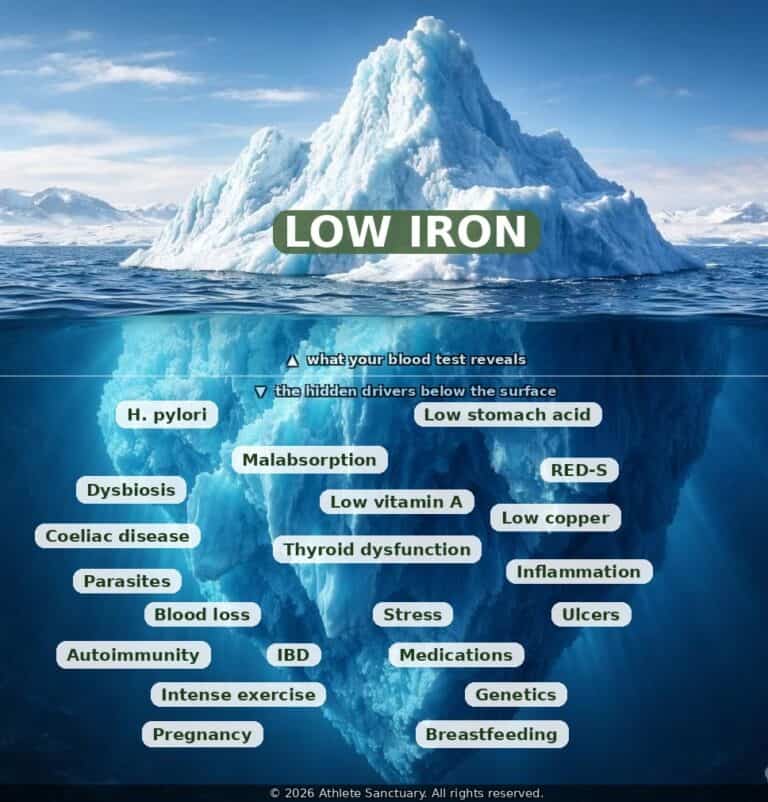
Iron deficiency is one of the most common nutritional issues we see in athletes across all sports, all genders and all levels of competition.1 But iron itself is rarely the whole story. Like an iceberg, what shows up on a blood test is only the visible tip.
Below the surface lies a deeper set of questions: why is iron low? What is making it hard to absorb, store or use? Until those questions are answered, supplementation is often little more than filling a bucket with a hole still in it.
Here are five of the most common myths we encounter and what the research actually tells us.
Diet absolutely matters. But if the issue is absorption rather than intake, adding more steak or spinach to your plate will not move the needle. Iron requires a highly acidic environment to be absorbed in the small intestine.
Low stomach acid (hypochlorhydria), gut dysbiosis, intestinal parasites such as Giardia or H. pylori, coeliac disease, or long-term stress can all quietly undermine your ability to absorb the iron you eat. Identifying and addressing the root cause, not just the dietary source, is where recovery begins.2
Anaemia is the end stage of iron deficiency, not the beginning. Long before haemoglobin drops, falling ferritin levels begin to impair oxygen transport, muscle metabolism and cognitive function. Research confirms that endurance performance can decline by 3–4% in iron-deficient but non-anaemic female athletes, with improvements of 20% observed after supplementation.3
For endurance athletes in particular, the evidence now supports a ferritin threshold of at least 50 µg/L well above the 30 µg/L commonly listed as the lower reference on a standard blood panel.4
This one can actually backfire. A single large oral dose of iron triggers a spike in hepcidin, the hormone that regulates iron absorption which suppresses uptake from the very next dose for up to 24–48 hours.5 More frequent, higher doses do not mean more iron reaches your cells. If imbalances already exist between iron, zinc and copper, more iron can actually make things worse.

Current research supports alternate-day supplementation taken in the morning when hepcidin levels are naturally at their lowest, paired with vitamin C, and well away from coffee, calcium and hard training sessions.2,5
Standard laboratory reference ranges are built around the general population, not athletes under high training loads. A ferritin reading that looks acceptable in a sedentary adult may represent a meaningful deficit for a runner clocking 80-kilometre weeks or a swimmer in twice-daily training.
Iron status also shifts with training load, illness, altitude exposure, hormonal cycles and energy availability, meaning a single annual test provides a very incomplete picture.1,6
Aim to test at least twice a year and more often if you are iron deficient, approaching altitude, or increasing training load significantly.
This is perhaps the most important myth of all. Iron deficiency in athletes rarely exists in isolation. Relative Energy Deficiency in Sport (REDs), a state of chronically low energy availability is strongly associated with impaired iron status, as the body down-regulates non-essential processes, including nutrient absorption, when fuel is scarce.7
Thyroid dysfunction, including subclinical hypothyroidism, is closely linked to both low stomach acid and altered iron metabolism so individuals with iron deficiency can have significantly lower levels of thyroid hormones FT3 and FT4.8
Genetics can also provide useful understanding around iron mobilisation and iron requirements as detected in our myDNA Comprehensive Health Report. Underlying infections such as H. pylori or intestinal parasites compete directly with the host for available iron and can make supplementation entirely ineffective until the infection is resolved.2